Asbestos: Asbestos can cause a variety of lung
disease from benign pleural plaques tomesothelioma.
Pleural plaques
Pleural plaques are benign and do not undergo malignant change. They are the
most common form of asbestos related lung disease and generally occur after a
latent period of 20-40 years.
Pleural thickening
Asbestos exposure may cause diffuse pleural thickening in a similar pattern to
that seen following an empyema or haemothorax. The underlying pathophysiology
is not fully understood.
Asbestosis
The severity of asbestosis is related to the length of exposure. This is in
contrast to mesothelioma where even very limited exposure can cause disease.
The latent period is typically 15-30 years. Asbestosis typically causes lower
lobe fibrosis. As with other forms of lung fibrosis the most common symptoms
are shortness-of-breath and reduced exercise tolerance.
Mesothelioma
Mesothelioma is a malignant disease of the pleura. Crocidolite (blue) asbestos
is the most dangerous form.
Possible features
progressive shortness-of-breath
chest pain
pleural effusion
Patients are usually offered palliative chemotherapy and there is also a
limited role for surgery and radiotherapy. Unfortunately the prognosis is very
poor, with a median survival from diagnosis of 8-14 months.
Lung cancer
Asbestos exposure is a risk factor for lung cancer and also has a synergistic effect
with cigarette smoke.
Aspergilloma
An aspergilloma is a fungus ball which often colonises an existing lung cavity
(e.g. secondary to TB, lung cancer or cystic fibrosis)
Hypertension in pregnancy NICE published guidance in 2010 on the management of hypertension in pregnancy. They also made recommendations on reducing the risk of hypertensive disorders developing in the first place. Women who are at high risk of developing pre-eclampsia should take aspirin 75mg od from 12 weeks until the birth of the baby. High risk groups include:
hypertensive disease during previous pregnancies chronic kidney disease autoimmune disorders such as SLE or antiphospholipid syndrome type 1 or 2 diabetes mellitus The classification of hypertension in pregnancy is complicated and varies. Remember, in normal pregnancy: blood pressure usually falls in the first trimester (particularly the diastolic), and continues to fall until 20-24 weeks after this time the blood pressure usually increases to pre-pregnancy levels by term Hypertension in pregnancy in usually defined as: systolic > 140 mmHg or diastolic > 90 mmHg or an increase above booking readings of > 30 mmHg systolic or > 15 mmHg diastolic After establishing that the patient is hypertensive they should be categorized into one of the following groups: Watch This Video:
A=Pre-existing hypertension :
A history of hypertension before pregnancy or an elevated blood pressure > 140/90 mmHg before 20 weeks gestation No proteinuria, no oedema Occurs in 3-5% of pregnancies and is more common in older women B=Pregnancy-induced HTN (PIH, also known as gestational HTN): Hypertension (as defined above) occurring in the second half of pregnancy (i.e. after 20 weeks) No proteinuria, no oedema Occurs in around 5-7% of pregnancies Resolves following birth (typically after one month). Women with PIH are at increased risk of future pre-eclampsia or hypertension later in life C=Pre-eclampsia: Pregnancy-induced hypertension in association with proteinuria (> 0.3g / 24 hours) Oedema may occur but is now less commonly used as a criteria Occurs in around 5% of pregnancies Pre-eclampsia - Pre-eclampsia is a condition seen after 20 weeks gestation characterised by: Watch This Video:
Pregnancy-induced hypertension in association with Proteinuria (> 0.3g / 24 hours). Oedema used to be third element of the classic triad but is now often not included in the definition as it is not specific Pre-eclampsia is important as it predisposes to the following problems: fetal: prematurity, intrauterine growth retardation eclampsia haemorrhage: placental abruption, intra-abdominal, intra-cerebral cardiac failure multi-organ failure Risk factors:
> 40 years old nulliparity (or new partner) multiple pregnancy body mass index > 30 kg/m^2 diabetes mellitus pregnancy interval of more than 10 years family history of pre-eclampsia previous history of pre-eclampsia pre-existing vascular disease such as hypertension or renal disease Features of severe pre-eclampsia: hypertension: typically > 170/110 mmHg and proteinuria as above proteinuria: dipstick ++/+++ headache visual disturbance papilloedema RUQ/epigastric pain hyperreflexia platelet count < 100 * 106/l, abnormal liver enzymes or HELLP syndrome Management: Management: consensus guidelines recommend treating blood pressure > 160/110 mmHg although many clinicians have a lower threshold Oral labetalol is now first-line following the 2010 NICE guidelines. Nifedipine and hydralazine may also be used Delivery of the baby is the most important and definitive management step. The timing depends on the individual clinical scenario Eclampsia Eclampsia may be defined as the development of seizures in association pre-eclampsia. To recap, pre-eclampsia is defined as: 1) condition seen after 20 weeks gestation 2) pregnancy-induced hypertension 3) proteinuria
Magnesium sulphate is used to both prevent seizures in patients with severe pre-eclampsia and treat seizures once they develop. Guidelines on its use suggest the following: 1) should be given once a decision to deliver has been made 2) in eclampsia an IV bolus of 4g over 5-10 minutes should be given followed by an infusion of 1g / hour 3) urine output, reflexes, respiratory rate and oxygen saturations should be monitored during treatment 4) treatment should continue for 24 hours after last seizure or delivery (around 40% of seizures occur post-partum) Other important aspects of treating severe pre-eclampsia/eclampsia include fluid restriction to avoid the potentially serious consequences of fluid overload Centrally acting antihypertensives Examples of centrally acting antihypertensives include: methyldopa: used in the management of hypertension during pregnancy moxonidine: used in the management of essential hypertension when conventional antihypertensives have failed to control blood pressure clonidine: the antihypertensive effect is mediated through stimulating alpha-2 adrenoceptors in the vasomotor centre
Hypertention Secondary causes: It is thought that between 5-10% of patients diagnosed with hypertension have primary hyperaldosteronism, including Conn's syndrome. This makes it the single most common cause of secondary hypertension.
Renal disease accounts for a large percentage of the other cases of secondary hypertension. Conditions which may increase the blood pressure include: glomerulonephritis pyelonephritis adult polycystic kidney disease renal artery stenosis
Endocrine disorders (other than primary hyperaldosteronism) may also result in increased blood pressure: phaeochromocytoma Cushing's syndrome Liddle's syndrome congenital adrenal hyperplasia (11-beta hydroxylase deficiency) acromegaly Other causes include: NSAIDs pregnancy coarctation of the aorta the combined oral contraceptive pill steroids MAOI 3- Isolated systolic hypertension Isolated systolic hypertension (ISH) is common in the elderly, Affecting around 50% of people older than 70 years old. The Systolic Hypertension in the Elderly Program (SHEP) back in 1991 established that treating ISH reduced both strokes and ischaemic heart disease. Drugs such as thiazides were recommended as first line agents. This approach is contradicated by the 2011 NICE guidelines which recommends treating ISH in the same stepwise fashion as standard hypertension. Hypertension diagnosis: NICE published updated guidelines for the management of hypertension in 2011. Some of the key changes include: classifying hypertension into stages recommending the use of ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM) Why were these guidelines needed? It has long been recognised by doctors that there is a subgroup of patients whose blood pressure climbs 20 mmHg whenever they enter a clinical setting, so called 'white coat hypertension'. If we just rely on clinic readings then such patients may be diagnosed as having hypertension when the vast majority of time there blood pressure is normal. This has led to the use of both ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM) to confirm the diagnosis of hypertension. These techniques allow a more accurate assessment of a patients' overall blood pressure. Not only does this help prevent overdiagnosis of hypertension - ABPM has been shown to be a more accurate predictor of cardiovascular events than clinic readings. Blood pressure classification: This becomes relevant later in some of the management decisions that NICE advocate. Stage Criteria Stage 1 hypertension Clinic BP >= 140/90 mmHg and subsequent ABPM daytime average or HBPM average BP >= 135/85 mmHg Stage 2 hypertension Clinic BP >= 160/100 mmHg and subsequent ABPM daytime average or HBPM average BP >= 150/95 mmHg Severe hypertension Clinic systolic BP >= 180 mmHg, or clinic diastolic BP >= 110 mmHg 4- Diagnosing hypertension:
Firstly, NICE recommend measuring blood pressure in both arms when considering a diagnosis of hypertension. If the difference in readings between arms is more than 20 mmHg then the measurements should be repeated. If the difference remains > 20 mmHg then subsequent blood pressures should be recorded from the arm with the higher reading. It should of course be remember that there are pathological causes of unequal blood pressure readings from the arms, such as supravalvular aortic stenosis. It is therefore prudent to listen to the heart sounds if a difference exists and further investigation if a very large difference is noted. NICE also recommend taking a second reading during the consultation, if the first reading is > 140/90 mmHg. The lower reading of the two should determine further management. NICE suggest offering ABPM or HBPM to any patient with a blood pressure >= 140/90 mmHg. If however the blood pressure is >= 180/110 mmHg: immediate treatment should be considered if there are signs of papilloedema or retinal haemorrhages NICE recommend same day assessment by a specialist NICE also recommend referral if a phaeochromocytoma is suspected (labile or postural hypotension, headache, palpitations, pallor and diaphoresis) Ambulatory blood pressure monitoring (ABPM): at least 2 measurements per hour during the person's usual waking hours (for example, between 08:00 and 22:00) use the average value of at least 14 measurements If ABPM is not tolerated or declined HBPM should be offered. Home blood pressure monitoring (HBPM): for each BP recording, two consecutive measurements need to be taken, at least 1 minute apart and with the person seated BP should be recorded twice daily, ideally in the morning and evening BP should be recorded for at least 4 days, ideally for 7 days discard the measurements taken on the first day and use the average value of all the remaining measurements Interpreting the results 1) ABPM/HBPM >= 135/85 mmHg (i.e. stage 1 hypertension) treat if < 80 years of age AND any of the following apply; target organ damage, established cardiovascular disease, renal disease, diabetes or a 10-year cardiovascular risk equivalent to 20% or greater 2) ABPM/HBPM >= 150/95 mmHg (i.e. stage 2 hypertension) offer drug treatment regardless of age 5- Hypertension management: NICE published updated guidelines for the management of hypertension in 2011. Some of the key changes include: classifying hypertension into stages recommending the use of ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM) calcium channel blockers are now considered superior to thiazides bendroflumethiazide is no longer the thiazide of choice Managing hypertension 1) Lifestyle advice should not be forgotten and is frequently tested in exams: A low salt diet is recommended, aiming for less than 6g/day, ideally 3g/day. The average adult in the UK consumes around 8-12g/day of salt. A recent BMJ paper* showed that lowering salt intake can have a significant effect on blood pressure. For example, reducing salt intake by 6g/day can lower systolic blood pressure by 10mmHg caffeine intake should be reduced the other general bits of advice remain: stop smoking, drink less alcohol, eat a balanced diet rich in fruit and vegetables, exercise more, lose weight 2) ABPM/HBPM >= 135/85 mmHg (i.e. stage 1 hypertension) treat if < 80 years of age AND any of the following apply; target organ damage, established cardiovascular disease, renal disease, diabetes or a 10-year cardiovascular risk equivalent to 20% or greater 3) ABPM/HBPM >= 150/95 mmHg (i.e. stage 2 hypertension) offer drug treatment regardless of age For patients < 40 years consider specialist referral to exclude secondary causes. Step 1 treatment: patients < 55-years-old: ACE inhibitor (A) patients > 55-years-old or of Afro-Caribbean origin: calcium channel blocker Step 2 treatment: ACE inhibitor + calcium channel blocker (A + C) Step 3 treatment: add a thiazide diuretic (D, i.e. A + C + D) NICE now advocate using either: chlorthalidone (12.5-25.0 mg once daily) or indapamide (1.5 mg modified-release once daily or 2.5 mg once daily) in preference to a conventional thiazide diuretic such as bendroflumethiazide 6- NICE define a clinic BP >= 140/90 mmHg after step 3 treatment with optimal or best tolerated doses as resistant hypertension. They suggest step 4 treatment or seeking expert advice Step 4 treatment: 1) consider further diuretic treatment if potassium < 4.5 mmol/l add spironolactone 25mg od if potassium > 4.5 mmol/l add higher-dose thiazide-like diuretic treatment 2) if further diuretic therapy is not tolerated, or is contraindicated or ineffective, consider an alpha- or beta-blocker Patients who fail to respond to step 4 measures should be referred to a specialist. NICE recommend: If blood pressure remains uncontrolled with the optimal or maximum tolerated doses of four drugs, seek expert advice if it has not yet been obtained. Blood pressure targets Age < 80 years, Clinic BP 140/90 mmHg, ABPM / HBPM 135/85 mmHg Age > 80 years, Clinic BP 150/90 mmHg , ABPM / HBPM 145/85 mmHg New drugs: Direct renin inhibitors: e.g. Aliskiren (branded as Rasilez) by inhibiting renin blocks the conversion of angiotensinogen to angiotensin I No trials have looked at mortality data yet. Trials have only investigated fall in blood pressure. Initial trials suggest aliskiren reduces blood pressure to a similar extent as angiotensin converting enzyme (ACE) inhibitors or angiotensin-II receptor antagonists adverse effects were uncommon in trials although diarrhoea was occasionally seen only current role would seem to be in patients who are intolerant of more established antihypertensive drugs 7- Malignant hypertension Basics: severe hypertension (e.g. >200/130 mmHg) occurs in both essential and secondary types fibrinoid necrosis of blood vessels, leading to: retinal haemorrhages, exudates, and proteinuria, haematuria due to renal damage (benign nephrosclerosis). can lead to cerebral oedema → encephalopathy Features: classically: severe headaches, nausea/vomiting, visual disturbance however chest pain and dyspnoea common presenting symptoms papilloedema severe: encephalopathy (e.g. seizures) Management: reduce diastolic no lower than 100mmHg within 12-24 hrs bed rest most patients: oral therapy e.g. atenolol if severe/encephalopathic: IV sodium nitroprusside/labetolol
A bone marrow biopsy is really a process that takes a tiny sample from the marrow within your bones for examining inside a laboratory. This kind of test can be used to determine if you have an infection, disease, and , or other problems in your bone marrow.
Marrow has the two reliable and liquid elements. If the solid part of the bone is sampled, this is often named a biopsy. Aspiration is the technique utilized to acquire the liquid a part of the marrow.
Bone marrow could be the spongy tissue found out inside your bones. From the much larger bones- like your spine, breastbone, hips, ribs, legs, or skull-bone marrow involves cells in which make white blood cells, Red blood cells, too as platelets. Your very own white blood cells aids in preventing infection, your Red blood cells carry oxygen also nutrition, whilst your platelets stimulate the blood to clot
Troubles with bone marrow can develop lasting, significant well being worries. A bone marrow biopsy is among a lot of tests which can be done to examine the cells of the bone marrow for difficulties or diseases.
Why Is a Bone Marrow Biopsy Done?
If blood screeningexhibitloweramounts of platelets or white or red blood
cells, your physician may
possibly order a bone marrow biopsy.
Problemsas well asillnessesthat couldaffect your
bone marrowinclude:
1- Anemia,all types
2- bone marrow diseases, such as myelofibrosis or myelodysplastic syndrome
3- blood cell illnesses, like as leukopenia or polycythemia
4- cancers of the bone marrow or blood, like as leukemias or lymphomas
5- hemochromatosis, a genetic disorder in which iron builds in the blood
infection, such as sepsis
NB.
A bone marrow biopsy can be a crucial take a look at should you be undergoing cancer treatment, as it might help identify if the most cancers has unfold in your bones
Risks of a Bone Marrow Biopsy
On the other hand in some uncommon situations, the following complications are probable:
A- allergic reaction to anesthesia
B- excessive bleeding
C- infection
D- long-lasting discomfort at the spot exactly where the biopsy was taken
These dangers are rare and most generally take place among individuals who have other situations that weaken their immune systems or decrease their platelet counts
How to Prepare for a Bone Marrow Biopsy?
Your medical doctor will carry out various examinations prior to the biopsy. Through these tests, be sure to tell your physician about any medications you take-including over-the-counter medicines or nutritional supplements-and any known allergies you have got.
Your doctor may possibly ask you to stop taking specific medicines prior to the process. By no means stop taking a medication unless your medical professional instructs you to complete so.
Tell your medical doctor should you be nervous. He or she may well give you a mild sedative that will help you via your process.
Stick to all of your doctor’s instructions before the process. Usually do not overlook to show up on time for your biopsy. You might also choose to arrange to get a ride dwelling.
How a Bone Marrow Biopsy Is Performed?
you will be asked to alter into a hospital gown, Ahead of the test. Then you will stay in your part or rest in your tummy in a area exactly where the process is going to take place.
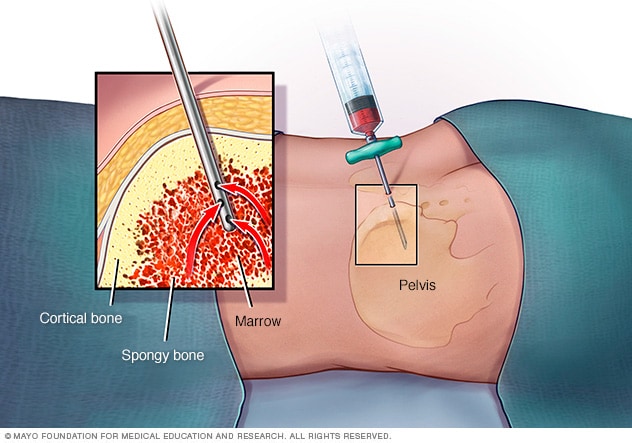
A doctor or registered nurse will provide you with a nearby sedation to numb the location exactly where the biopsy is going to be used. Usually this may be at the major ridge of your back end hipbone. Occasionally it might be studied from your upper body bone fragments.
You might really feel a brief sting as the anesthesia is injected.
Your medical professional is likely to make a modest cut so a hollow needle can easily get previous the facial skin. The needle then will go in to the bone tissue. It records a cylinder-formed test recognized like a primary sample.
According to the National Institutes of Overall health, some individuals feel a dull discomfort or discomfort because the biopsy is taken, since the inside of the bones cannot be numbed. the Federal Organizations of Wellness, a number of people feel a uninteresting pain or soreness because the biopsy is taken, considering the fact that the inside of the bones can not be numbed, . Even so, not every person will experience this. (NIH, 2010)
Right away following the process, the cut might be bandaged, and you will be used into one more area to relax just before going home.
After a Bone Marrow Biopsy
You could feel some slight discomfort for about per week just after the procedure. That is easily managed with over-the-counter pain relievers. You are going to also need to care for the incision wound, which includes maintaining it dry for 24 hours following the biopsy.
When you happen to be caring for the wound, your bone marrow sample is going to be sent to a laboratory for testing. When the outcomes are back, your doctor may possibly contact you or have you come to their workplace to get a follow-up appointment to talk about the findings.
Abnormal results may be as a result of cancer, anemia, or an additional condition. Your physician may require to order far more tests to confirm a diagnosis or to determine how far the condition has gone. She or he will discuss your treatment options with you and enable you to strategy your subsequent measures during your follow-up appointment.












 9:22 AM
9:22 AM
 Unknown
Unknown